
Understanding MRI Staging of Rectal Cancer: T3c N2a Example
Case Overview
MRI assessment of a mid-rectal mass utilizing high-resolution T2 and Diffusion Weighted Imaging (DWI).
Technique
Multiplanar, multisequence imaging of the Rectum using following sequences. Axial diffusion weighted imaging with b-values 50, 400, and 800 s/mm2 and ADC map. IV contrast bolus administered by power injector followed by saline chase. Pre and post contrast T1 FS sequences. Full-pelvis post-contrast T1-weighted imaging. Previous Biopsy: None
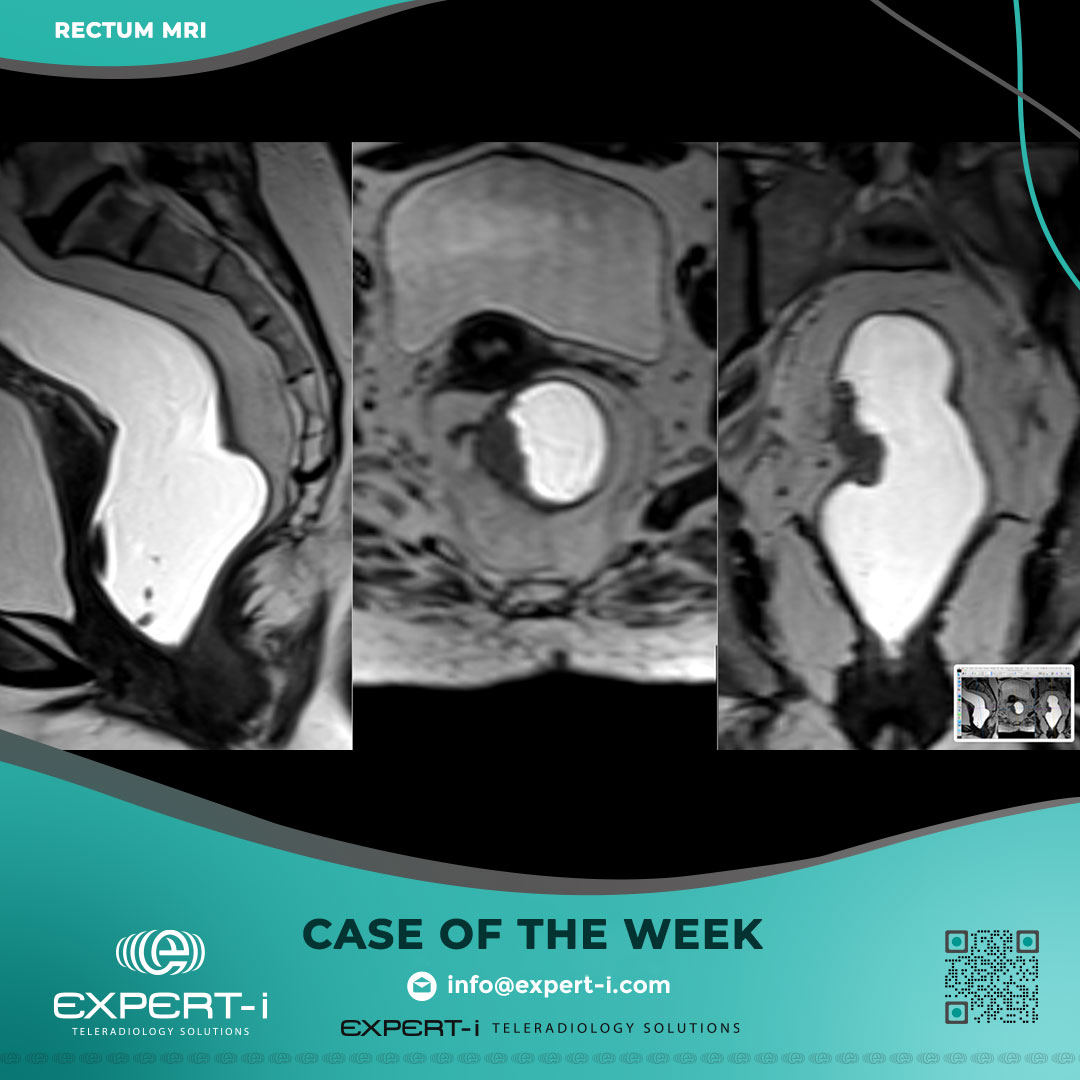
Findings
Tumor location and characteristics i. Tumor Location (lower edge from anorectal junction): Mid rectal ii. Distance from anal verge to distal tumor margin: 8.5cm. iii. Distance of lowest extent of tumor from top of anal sphincter: 5 cm iv. Craniocaudal length of the tumor: 3.6 cm v. Clock face of tumor: 7 o’clock to 11 o’clock. vi. Mucinous: No. vii. Tumor at or below the puborectalis sling: No. viii. Relationship to the anterior peritoneal reflection: (straddles).
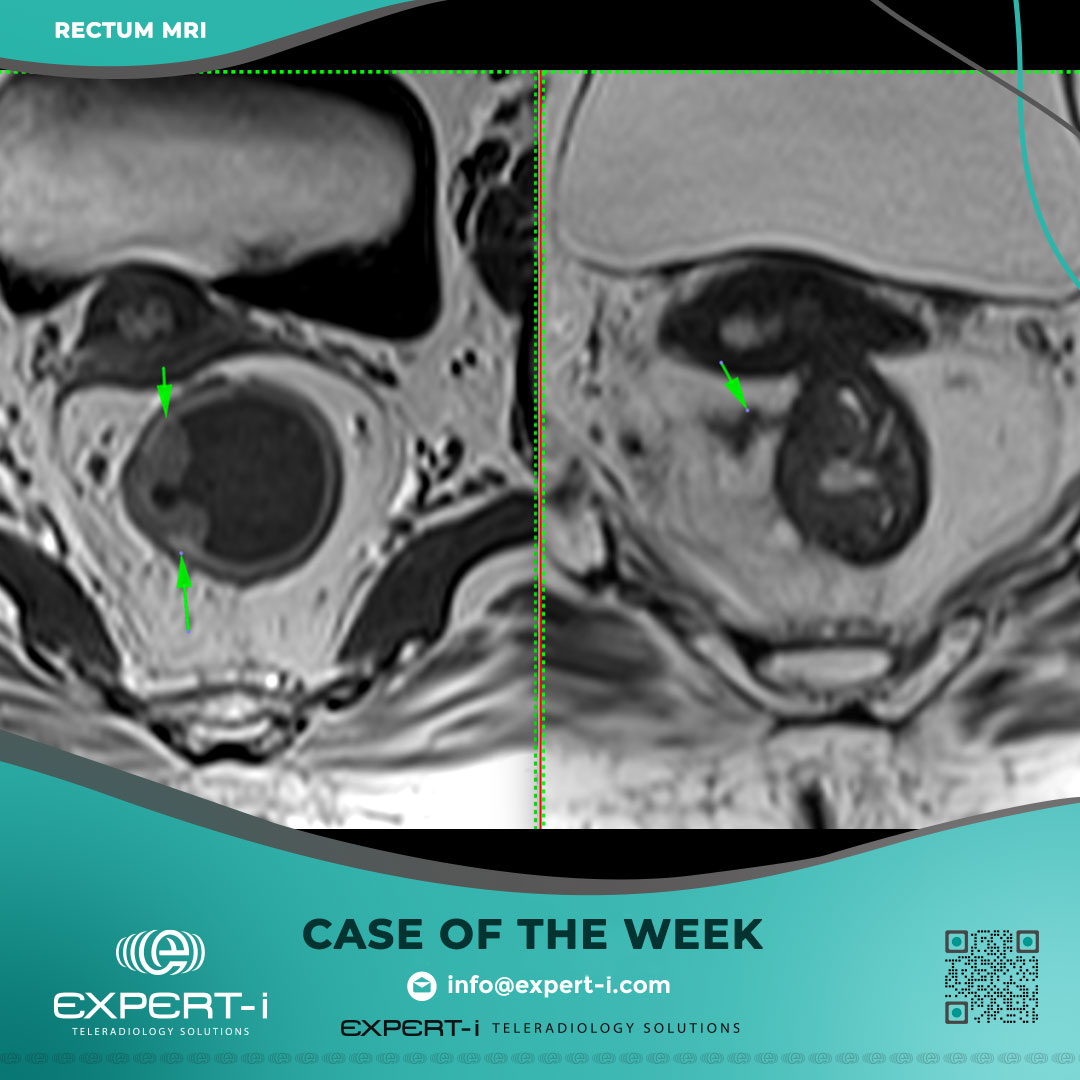
Extramural depth of invasion and MR T-category i. Extramural depth of invasion: 6 mm ii. T category: early T3 (T3c). iii. Invaded structures (for T4 tumors): None
Anal canal involvement: • Absent
Relationship of the tumor to mesorectal fascia (MRF) • Shortest distance between definitive tumor border to the MRF or Levator is: o 10 mm at 9 O’clock • Tumour spiculations close to the MRF: No
Extramural venous invasion • Extramural Venous Invasion (EMVI): Positive at 10 O’clock
Mesorectal lymph nodes and tumour deposits • Suspicious mesorectal lymph nodes/tumor deposits: Positive; 4 in number identified averaging 5mm in diamter
Extramesorectal lymph nodes • Suspicious extramesorectal lymph nodes: Absent
Other findings (complications, metastases, limitations): None
IMPRESSION
• Imaging-based staging is: T3cN2a
• MRI features impressive of mid rectal cancer
• Imaging based staging is: T3cN2a
• CRM is Clear. EMVI: Positive
Discussion & Learning Points
The strength of a structured report lies in its ability to provide the surgeon with actionable data. Here is a breakdown of the key terms found in this case:
1. Understanding T3 Sub-Staging (T3c)
In MRI staging of rectal cancer, a “T3” tumor has broken through the bowel wall (muscularis propria) and entered the mesorectal fat. However, not all T3s are the same. We use the ESMO Guidelines to sub-classify them by measuring the exact depth of invasion:
T3a: < 1 mm invasion
T3b: 1–5 mm invasion
T3c: 5–15 mm invasion (This patient measured 6 mm)
T3d: > 15 mm invasion Why it matters: T3c tumors carry a higher risk of recurrence than T3a/b and often require more aggressive neoadjuvant therapy.
2. What is EMVI?
Extramural Venous Invasion (EMVI) refers to the presence of tumor cells within the veins outside the rectal wall.
In this report, EMVI was Positive at the 10 o’clock position.
Clinical Impact: MRI-detected EMVI (mrEMVI) is an independent poor prognostic factor. It correlates with a significantly higher rate of distant metastasis (particularly to the liver) and local failure.
3. The CRM (Circumferential Resection Margin)
This is arguably the most important measurement for the surgeon. It measures the distance between the tumor (or malignant node) and the mesorectal fascia (the surgical envelope).
Clear CRM: > 1 mm distance.
Involved CRM: ≤ 1 mm distance.
This Case: The distance was 10 mm, meaning the CRM is Clear. This suggests a standard Total Mesorectal Excision (TME) surgery should result in clean margins (R0 resection).
4. N-Staging (N2a)
The “N” stage refers to lymph nodes.
N1: Metastasis in 1–3 regional lymph nodes.
N2a: Metastasis in 4–6 regional lymph nodes.
This patient had 4 suspicious nodes, pushing them into the N2a category, which signifies locally advanced disease.
Need Specialist Reporting?
Rectal cancer staging requires high-precision measurement that general reporting often misses. Expert-i consultants use verified structured templates to ensure every prognostic factor is captured.